Last updated: March 20, 2026
Contributors: FACS Team
Lead in drinking water is a serious issue because it can harm health even at low levels. The practical challenge is that people often get a lab report showing a number in ppb and then ask: “Is this safe?” This guide explains what ppb means, how the major standards are used, why results vary building to building, and how to respond based on what you found.
Key takeaways
- ppb (parts per billion) is a standard reporting unit for lead in water. In water testing, 1 ppb is essentially the same as 1 µg/L.
- The EPA’s health goal (MCLG) for lead is 0 ppb because there is no known safe level of exposure.
- The commonly cited 15 ppb value is an action level framework used in public water system compliance, not a “safe/not safe” line for individual fixtures in a building.
- The right response depends on where the sample came from, how it was collected (first-draw vs flushed), and whether you’re managing risk for vulnerable populations.
What “PPB” means on a water test report
PPB stands for parts per billion. In drinking water reports, it’s a way to express a very small concentration of a substance—like lead—in water.
In practice, many labs report lead as µg/L (micrograms per liter). For water, the conversion is straightforward:
- 1 ppb ≈ 1 µg/L
So if a result reads 10 ppb, that’s roughly 10 µg/L.
Why “safe lead level” is the wrong question
With lead, the best framing is not “safe vs unsafe.” The better framing is:
- What does this level mean for exposure risk in this specific building and fixture?
- What action is reasonable based on how the water is used and who is consuming it?
The EPA sets the Maximum Contaminant Level Goal (MCLG) for lead at 0 ppb because the agency’s position is that there is no safe level of exposure.
That does not mean every detection equals an emergency. It means any detection should be treated as a signal to interpret results carefully and, when warranted, reduce exposure.
Lead standards and benchmarks: a quick table
Different benchmarks get mixed together online. Here’s a clean way to keep them straight.
| Benchmark | Value | Applies to | What it means in practice |
| EPA MCLG (health goal) | 0 ppb | Public health goal | Non-enforceable goal reflecting no known safe exposure. |
| EPA Lead and Copper Rule framework (commonly cited “action level”) | 15 ppb | Public water systems (compliance sampling at the tap) | A compliance trigger tied to required actions and treatment technique requirements; not a “safe line” for a single fixture result. |
| FDA bottled water lead limit | 5 ppb | Bottled water | FDA standard for bottled water; commonly referenced as a comparison point. |
A key point: benchmarks have different purposes. A health goal is not the same thing as a compliance trigger, and neither automatically tells you what to do with an individual faucet result inside a building.
Why lead shows up in building water even when the utility is “in compliance”
A common misconception is that lead in water means “the city water has lead.” Often, the bigger driver is premise plumbing—the building’s own components.
Typical sources include:
- Older service lines or connectors that contain lead
- Older solder and plumbing materials
- Brass fixtures or valves that can contribute lead, especially under certain water chemistry conditions
- Stagnation (water sitting in pipes overnight or during low-use periods)
Public water systems use corrosion control strategies to reduce lead release, but the risk inside a specific building can still vary widely based on plumbing age, fixture types, and water use patterns.
How lead in water is typically tested
If you want results you can actually act on, collection method matters.
First-draw vs flushed samples
- First-draw (often after 6–8 hours of no use):
Helps identify lead that may leach from the fixture and immediate plumbing during stagnation. Often the most informative for exposure risk at that tap. - Flushed sample (after running water for a period):
Can help differentiate fixture/premise sources from water coming from farther upstream.
Sampling strategy matters
If you’re responsible for a facility, the most defensible approach is not “one sample from one sink.” Here’s how to sample properly:
- Select high-use drinking fixtures
- Include fixtures used by vulnerable populations (children, pregnant people, patients)
- Use consistent collection timing (e.g., first-draw after a defined stagnation period)
- Build a simple map/log so you can compare results over time
Common pitfalls that create misleading results
- Sampling only one location and assuming it represents the building
- Mixing first-draw and flushed results without labeling them clearly
- Testing hot water (hot water can increase leaching and is not the usual drinking-water pathway)
- Not cleaning/inspecting faucet aerators (debris can bias results)
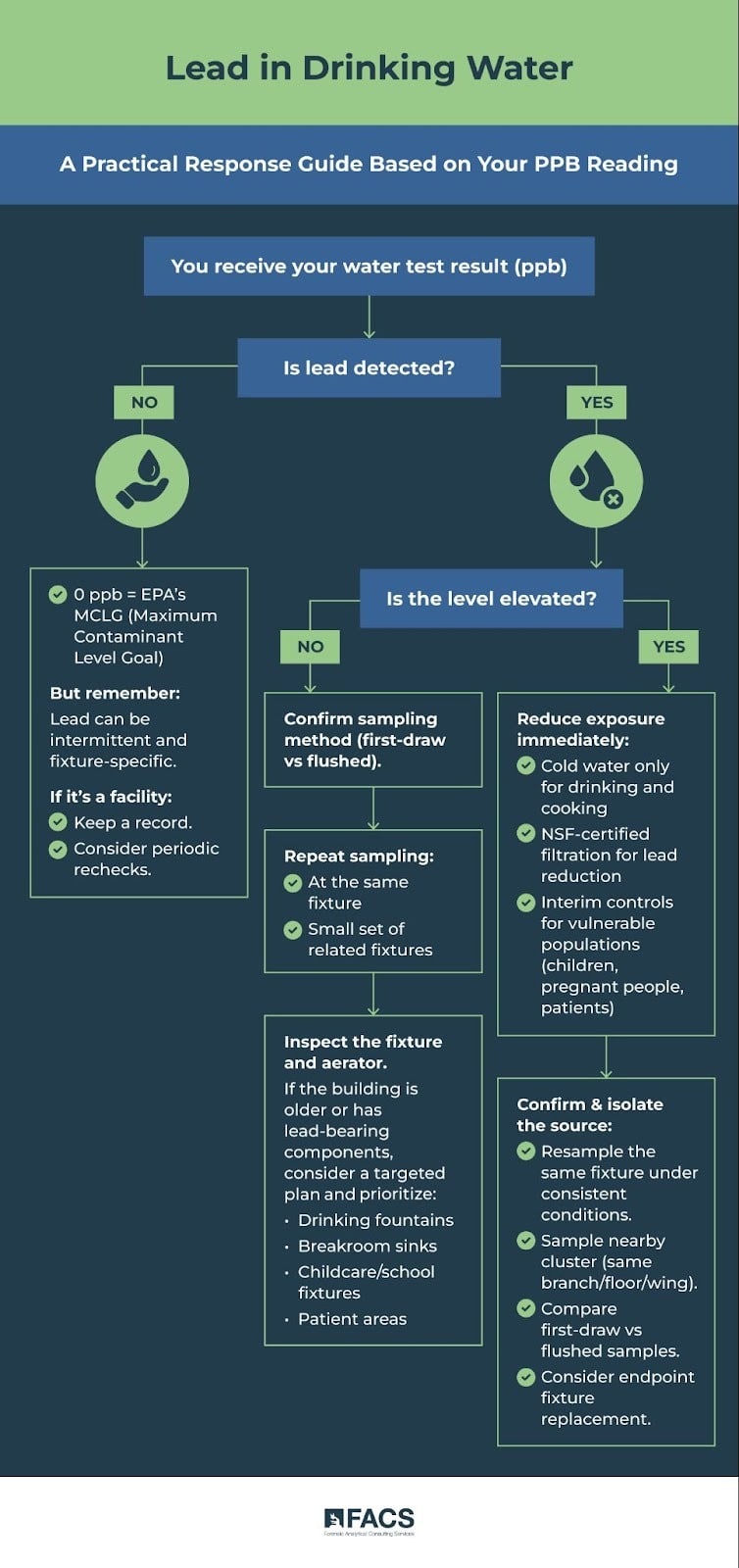

What to do with your result: a practical decision guide
Your response should match the measured level, the sampling method, and the exposure scenario.
If lead is non-detect
- Treat it as good news, but remember: lead can be intermittent and fixture-specific.
- If this is a facility, keep a record and consider periodic rechecks in a way that fits your risk profile and building changes (renovations, low-use periods, plumbing work).
If lead is detected but not “high”
This is where many buildings land.
- Confirm the sampling method (first-draw vs flushed).
- Consider repeat sampling at the same fixture and a small set of related fixtures.
- Inspect the fixture and aerator.
- If the building is older or has known lead-bearing components, consider a targeted plan: prioritize drinking fountains, breakroom sinks, childcare/school fixtures, and patient areas.
If lead is elevated
Focus on exposure reduction first, then source isolation.
- Use cold water only for drinking and cooking.
- Consider NSF-certified filtration specifically rated for lead reduction.
- If this is a facility serving children or other vulnerable populations, implement interim controls while you confirm results and identify sources.
Next, move into a structured “confirm and isolate” approach:
- Resample the same fixture under consistent conditions
- Sample a small cluster nearby (same branch line, same floor/wing)
- Compare first-draw vs flushed samples to locate the most likely source zone
- Consider fixture replacement where evidence points to the endpoint
Practical ways to reduce lead exposure
There are three categories of controls. The right choice depends on what the sampling shows.
1) Point-of-use filtration
For many buildings, this is the fastest exposure reduction tool.
- Pitcher, faucet-mount, or under-sink options can work if they are properly certified and maintained.
- Maintenance matters: cartridge change schedules are not optional.
2) Operational controls
These reduce stagnation-related peaks.
- Cold-water flushing protocols (especially after low-use periods)
- Putting rarely used fixtures on a scheduled use/flush plan
- Cleaning aerators on a routine basis (where appropriate)
3) Permanent corrective actions
- Replace high-lead fixtures
- Replace lead-containing premise plumbing components when identified
- Coordinate with utility programs where service line replacement is relevant
A note about vulnerable populations
Children and pregnant women are more vulnerable to lead exposure. Public health agencies emphasize minimizing exposure, and CDC guidance uses a blood lead reference value for identifying children with higher levels compared to most children—this is about prioritizing follow-up, not defining a “safe” blood lead level.
If your facility serves children (schools, childcare) or patients (healthcare), it is usually appropriate to treat “detectable lead” with a lower tolerance for ambiguity and a stronger emphasis on documentation and controls.
FAQ
What does ppb mean in a water test?
It’s a unit of concentration: parts per billion. In drinking water reporting, 1 ppb is essentially the same as 1 µg/L.
Is 15 ppb considered “safe”?
Not as a blanket statement. The 15 ppb value is commonly cited because of EPA Lead and Copper Rule compliance frameworks, but it is not a simple “safe/unsafe” line for a specific faucet result in a building.
Why is the health goal for lead zero?
EPA’s position is that there is no known safe level of exposure to lead, so the health goal (MCLG) is set at 0 ppb.
Should I test hot water?
Usually no. Use cold water for drinking and cooking, and test the water people actually consume.
Why do results vary from one faucet to another?
Because lead often comes from the fixture and nearby plumbing materials. Age, materials, stagnation time, and flow patterns can differ even within the same building.
What kind of filter reduces lead?
Look for filters that specifically state they reduce lead and that are certified to the appropriate drinking water standard for lead reduction. Follow the manufacturer’s cartridge replacement schedule.
How FACS can help
FACS supports organizations that need lead-in-water answers they can defend and implement:
- Sampling strategy: selecting locations and sample types that match the real exposure pathways
- Lab coordination and interpretation: turning numbers into a clear risk picture
- Practical corrective guidance: prioritizing fixes, interim controls, and retesting plans
If you have a lab report and want help interpreting what it means for your facility, contact FACS to discuss a practical path forward. Better yet, call FACS to have testing conducted for you.
In summary
- ppb is simply the reporting unit (1 ppb ≈ 1 µg/L).
- The EPA health goal for lead is 0 ppb because there is no known safe exposure level.
- Compliance benchmarks and “action levels” are not the same thing as a safety guarantee at an individual tap.
- The most useful next step is usually a simple, targeted sampling plan paired with practical exposure controls where warranted.
For more information call FACS at (888) 711-9998 or contact us online here: https://facs.com/contact-us/.